Cost effectiveness analysis in Japan – What’s changed?

Japan has historically been considered a key market for the pharmaceutical sector, with a rule-based pricing and reimbursement system, Japan was a “predictable” market which companies found attractive. However, there have been several policies recently introduced that have led to increasing price pressure on pharmaceuticals, including formalised cost effectiveness assessments (CEAs).
Cost effectiveness analysis for the purpose of public drug listing has been permitted by the Ministry of Health, Labour and Welfare (MHLW) in Japan for some time, dating back as far as 1992. The CEA data submission was previously voluntary and very little advice was given around its application or value. Very few pharmaceutical companies submitted a CEA as the data did not appear to influence the pricing or listing of new therapies entering the Country.
In 2012 the Centre for Outcomes Research and Economic Evaluation for Health (C2H) was founded and in 2016 C2H piloted the use of CEAs on a trial basis for a small number of products. After a series of consultations and refinement of the methodology, a consensus was reached, and a new CEA process was formally implemented in April 2019. Currently, the CEA is primarily used to adjust the price of already reimbursed therapies with an aim of making cost efficiencies and overall reduce healthcare expenditure.
Current pricing methodology
The pricing methodology in Japan are based on two methods:
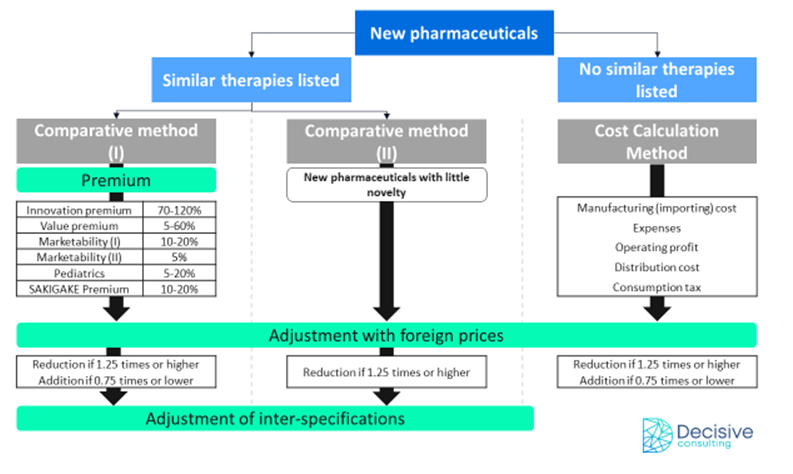
Figure 1: existing methods
The comparison methodology applies to products launching where there are similar therapies available and reimbursed within the same indication; If a therapy is superior vs. comparator, a premium is applied.
In the event of no comparable therapies being available, the price is determined through a cost calculation (mentioned above); here, the price is set based on manufacturing costs (or importation) and expected profits.
Where does CEA fit into the process?

Figure 2: CEA in the pathway
Upon determining a price the Central Social Insurance Medical Council (Chuikyo) will earmark specific medicines and medical devices for cost-effectiveness analysis. The selection process employs a five-tier system for decision-making:

For the category H3, there are no defined principles which constitute “notably high prices” and Chuikyo may opt for certain treatments if new clinical evidence could impact on the cost-effectiveness analysis or in cases where the prices are considered high.
Designated orphan diseases, haemophilia and HIV or paediatric products are exempt from cost-effectiveness analysis.
CEA adjustment rates

Figure 3: CEA Adjustment Rates
The ICER, which is based on the pilot program and the payer's willingness to pay (WTP), has been established at ¥5 million (~$37K USD). The price will remain unchanged if the ICER is less than ¥5 million per QALY, however, if the ICER falls between ¥5 million and ¥7.5 million (~$56K USD) the price adjustment rates for the utility premium and operating profit will gradually increase. The price will be adjusted at the maximum rate if the ICER exceeds ¥10 million (~$74K USD) per QALY.
Looking ahead
Despite the fact that CEAs are currently focused on listed products, if cost-effectiveness takes more of a prominent role in the HTA process at launch this could result in potential new challenges for pricing and market access in Japan.
Given that the HTA methodology in Japan is still in its relative infancy, it is expected to evolve further. Thus, it will be essential to keep a close eye on the developments in this space. Presently, the assessment process appears to be longer than that observed in other countries and moreover, only a handful of universities have been chosen as academic analysis groups, which poses a potential capacity challenge for the system when scaling.
The uncertainty around the selection of a particular product and when it will be selected also creates hurdles in preparing for commercialization. By implementing early planning and capacity assessment, organizations can ensure that they have sufficient resources to conduct CEAs effectively and efficiently. This proactive approach could help to avoid delays in conducting evaluations and ensure that the results are available when needed. It can also help organizations to optimize the use of available resources and ensure that the most critical evaluations receive the highest priority.
It is also suggested that Japan and South Korea are starting to refer to the prices of therapies that have been included in China's National Reimbursement Drug List (NRDL), albeit informally. The informal referencing of drug prices in China's NRDL by Japan and South Korea could have the potential to facilitate greater alignment between countries in Asia, and could even lead to a more collaborative approach to HTA, similar to that emerging in the EU. However, there may also be important political and economic factors that could influence the relative willingness of countries to collaborate on the assessment of technologies and innovation. Therefore, while there is potential for greater alignment and collaboration, it remains to be seen whether this will be realised in practice.
Written by Boon Yap